
What the paper reports
A 37-year-old woman had one MRI with gadolinium contrast. Her kidneys worked normally before the scan and stayed normal throughout — her eGFR was 100 before and 109 afterwards, which is well within the normal range.
Her urine was tested repeatedly over the following months. Gadolinium stayed above the lab's reference range (under 1.1 micrograms per 24 hours) for more than three months after the single dose. At the same time, gadolinium was not detectable in her blood — which is part of why the authors argue urine testing is the more useful measure once time has passed.
Two details are worth noticing. Her kidney function was normal, so this is not the situation that causes nephrogenic systemic fibrosis. And the agent she received, gadopiclenol, is a macrocyclic agent — the type that holds onto its gadolinium more tightly and is generally considered lower-risk than the older linear agents.
The timeline
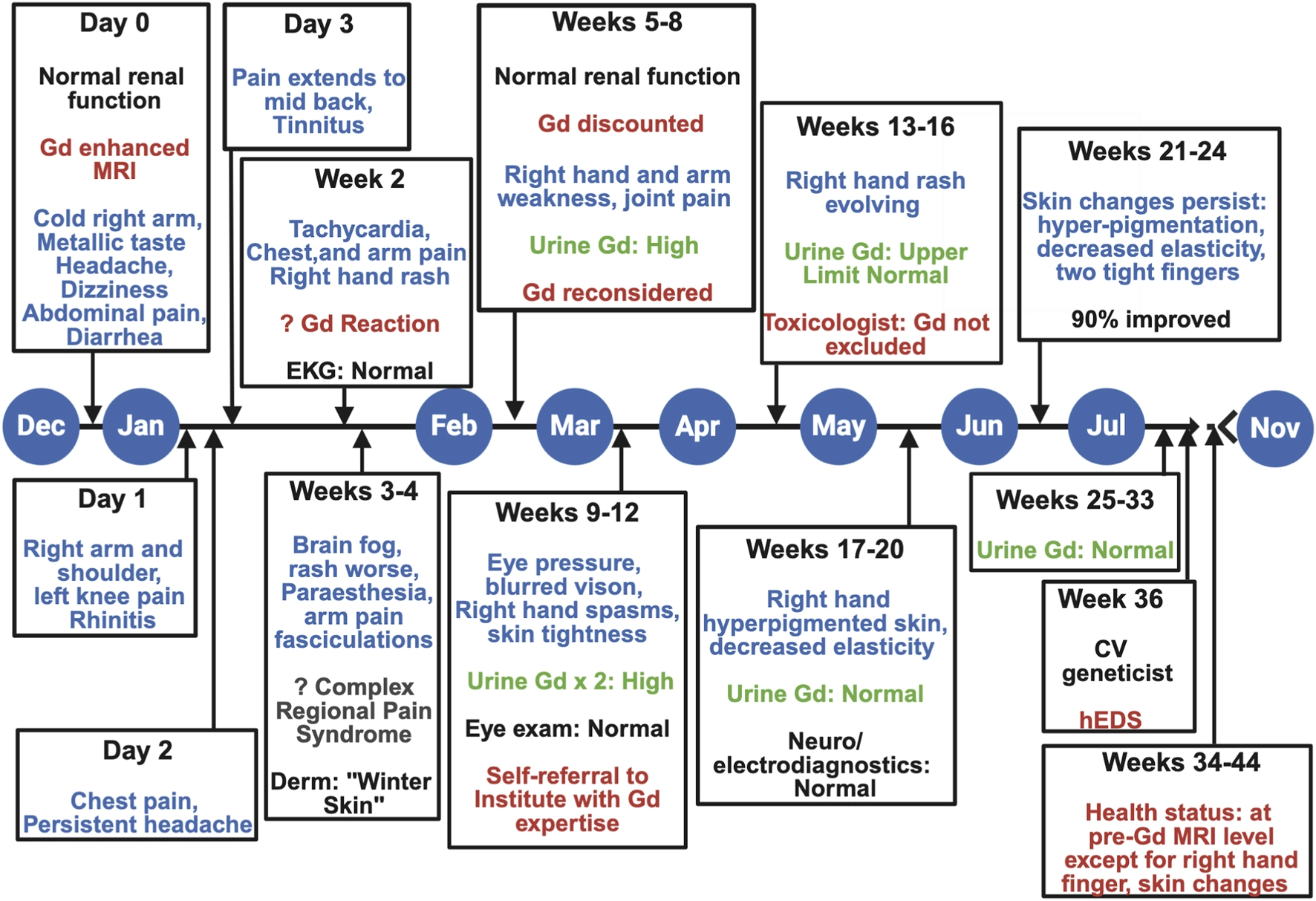
This is the course the authors documented, in their order.
Day 0
She had an MRI with a single 10 mL dose of gadopiclenol, injected into her right hand. Within hours she reported a cold arm, a metallic taste, headache, dizziness, abdominal pain, nausea and severe diarrhoea, then joint and limb pain.
Days 2–3
The first wave of symptoms settled, but the arm pain got worse and the headache stayed.
Week 3
Trouble concentrating and remembering, pain that moved around the body, pins and needles, and an "icy" sensation in the hand.
Week 5
First primary care visit. Fine pink marks on the upper arms, dry skin, and redness on the back of the right hand — the hand the contrast went into.
Months 1–6
Symptoms gradually improved and the urine gadolinium came back down to normal.
After that
Her health largely returned to where it was before the scan. Skin changes on the right hand partly remained, along with intermittent symptoms in that hand.
Where hEDS comes in
After most of her symptoms had settled, she was formally diagnosed with hypermobile Ehlers-Danlos syndrome (hEDS), a connective tissue condition. The authors raise the possibility that connective tissue biology might affect how a body responds to retained gadolinium.
They are careful about this, and so should we be: they call it speculative and say it has not been demonstrated in people with hEDS. If you have hEDS, this paper does not mean contrast will harm you.
What the authors say the case cannot answer
These limitations are the authors' own. They matter more than the findings, because they set what the case can be used for.
- No tissue was tested, so gadolinium retention in the body was never directly confirmed — the evidence is what was measured in urine.
- No skin biopsy was taken while the rash was active, and no kidney biopsy was done.
- Urinary creatinine was not measured, which is normally used to check that a 24-hour urine collection was complete.
- The patient was researching her own case and trying interventions on her own, which the authors say introduced bias and makes it harder to interpret what changed and why.
- No specific phenotype, mechanism, or validated biomarker was identified.
Read the original
This page is a summary. The paper is open access — you can read every word of it for free, including the parts we condensed.
Cox C, Unruh A, Wagner B, Escobar GP, Walsh C, Jastrzemski OX, Henderson I, DeAguero J. “Case Report: A hypothesis-generating case of gadolinium retention and persistent symptoms after MRI despite normal renal function in a patient with hypermobile Ehlers-Danlos syndrome.” Frontiers in Toxicology, volume 8 (2026).
Where to go next
Sources and Review
Author: Gadolinium.org Editorial Team (Patient-Led Education)
Last reviewed: July 17, 2026
How this page was reviewed: Summarized from the open-access paper cited below. Wording follows the authors’ own hedging, including their statement that causality cannot be established and that the hEDS link is speculative.
Clinician review: No physician has reviewed this page. It was checked by the editorial team against the sources listed below.
This page is for education only and is not a diagnosis or treatment plan.